In the 200 or so products I’ve worked with over the years, there have been some truly excellent strategic plans developed by the teams involved – cutting insight, opportunities and challenges uncovered, winning strategies innovated to meet them.
However, regardless of the quality of that strategic thinking, undoubtedly the greatest threat comes after their creation – in their capture and communication.
Inevitably it seems, these delicately nuanced arguments get boiled down into bullet points, charts and tables. In doing this, words and phrases that might challenge are replaced with the deliberately ambiguous. Important connections between insights and ideas are ripped apart and clumped in lists or abstract diagrams. Bullet points reign supreme.
We’re left with a strategic plan that is a pale semblance of the thought that went before. To the outside observer it appears to be largely generic and is hardly inspiring to senior stakeholders who must bless it, or to those who must ultimately implement it.
Sound familiar?
There is a better way - it’s called strategic narrative and it means capturing your strategy – with all of the nuances and interconnections - into a strategic “story”. Read more....
If there is any one thing we know in pharmaceutical marketing, it’s that the pressure to differentiate has never been greater; whether it’s with physicians to encourage change, or with payers to prove value.
We all say this, but do we really mean it? Do our organisations fully understand it, and do we “put our money where our mouth is”?
Here’s an edited version of a talk that marketing guru Seth Godin at TED (you can see the full talk here). I believe it superbly captures the nuanced reasons why we need to change our approach to product development and commercialisation.
Seth’s key point is that products can no longer just be very good or better, they need to be remarkable; what he would call a “purple cow”.
I believe this is superbly relevant in modern pharmaceuticals.
In developing products, so much of what we do is driven by attaining regulatory approval; which by it’s nature looks to measure products by established, often composite, parameters – like an ACR score in rheumatoid arthritis, or an Overall Survival score in oncology.
However, with so many disease areas now well served by existing treatments, being very good, or maybe even marginally better than what’s already out there is simply not good enough to warrant access from payers and adoption by prescribers. You need to be remarkable, or what the French Transparency Commission would call innovative.
This means that, for example, bringing yet another product to market for RA with a “TNF-like” ACR score is simply not good enough, regardless of how hard that benchmark is to attain. For products to succeed they must find a remarkable benefit backed by a plausible rationale applied to a discrete patient population.
While this has always been the formula for success, in the past products were able to succeed with only one or two of those three elements. Not anymore. If you want to tap into the Otaku that can break your product into a satisfied market, you need to give them something to be excited about.
To create such remarkable products there are two things that we need to do and Seth spells both of them out:
1) Employ better design With respect to the pharmaceutical industry this refers to the development programme. It means that instead of settling for what will secure regulatory approval (not necessarily easy in the first place) we need to go beyond and find other ways of communicating the remarkably different benefit that our product can provide within well defined patient groups. It means that just showing better FEV1 scores in respiratory or Relative Risk Reduction in cardiovascular disease is no longer enough; you need to find novel or unconventional parameters to express how what you’re bringing to the market is remarkably different.
No doubt this translates into extra cost and resource, as realistically this data needs to be generated in addition to what regulators will demand. It also requires more thought, planning and ingenuity to pick what those new parameters should be. However, that’s the modern cost of success, and as Seth says “Design is free when you get to scale” (i.e. the marginal cost of this is incidental compared to the value it creates).
2) Take more “risks” Spend more money on endpoints over and above what is required, and that are not guaranteed to add value.
Rather than bringing out a mass market product “for everyone” within a given disease area, create a medicine that will have Otaku; that will have greater benefit in smaller, discrete patient populations and that may at first only be adopted by sub segments of your customers. Flagrantly and intentionally risking, dare I say it, being niched (shock)!
But while his philosophy does have elements of inherent risk, it is by no means as risky as the conventional industry standard “safe” approach: to show that a new medicine is marginally better than what has gone before it on established parameters, and that it is appropriate for use in as many patients as possible.
This is modern pharmaceutical development suicide, yet lemming after lemming continues to line up.
If you were a payer, would you replace a functioning standard of care (SoC) in all your patients for a new premium priced product that was only marginally better? I suspect, that like many payers do, you would at best reserve it for use in SoC failures and look for patient sub-groups in which to restrict its usage.
If you were a clinician, would it really be worth braving the risks and hurdles of adopting a new product for one that is at best marginally better than what you already have and know? Even if you were an innovator, would the “safe” product I describe ignite the Otaku within you?
As Seth describes, the truth of this complex and cluttered modern world is that only Purple Cows that can ignite Otaku give themselves a chance to cut through and succeed. Is your ambition to be risky, or very good? The choice is yours.
Here's a great video that talks about the continued emergence of social media.
Even though it's 6 month old (an age on the social media trajectory), the facts and figures in it are eye-popping.
At this point, social media is still predominantly a tactical channel, but what I love about it is its ethos; customer driven (like diffusion), not promotional message driven. In effect the New vs the Old pharma marketing model.
Read more....
There’s an interesting debate that’s been ongoing about pharmaceutical companies’ approach to data publication. Unusually it’s actually spilled over into the mainstream media (BBC Radio 4 news) and is captured in a head to head article called Is the conflict of interest unacceptable when drug companies conduct trials on their own drugs? (BMJ 2009; 339:b4949 and b4953).
The protagonists of the argument are Ben Goldacre (arguing YES to the proposition) and Vincent Lawton (arguing NO). You can access their viewpoints via the hyperlink in each of their names.
Having heard yet another pharma spokesman be made to sound like a henchman of an evil empire on the radio, I had a closer look at each of their arguments. Read more....
When I talk with people about the New Pharmaceutical Marketing and how it's based on Diffusion of Innovation, they say "Hey, makes sense. Like it." It explains a lot of the problems that old pharma marketing couldn't tackle and gives us a way to attack many of the new ones.
My suspicion however, is that they may subconsciously think "But is this really totally proven, or is it a marketing fad? I mean, every one else is still doing it the old way."
"Diffusion of Innovation" sounds sexy, but it’s no passing fad. It is based on years of work around the laws of adoption of innovation, on the concepts laid out in Everett Rogers seminal book The Diffusion of Innovations.
While there is new thinking in today’s frameworks, the reality is that the enormous evidence base behind the ideas that we discuss is actually very well established. And, though it’s sometimes overlooked, a vast amount of the work we cite and build upon was conducted in medicine, in healthcare. Read more....
We all like to think about how we can encourage or speed up adoption of a brand or idea. What we rarely think about is how to stem the flow of people "de-adopting" or discontinuing it's use.
You only have to think about this if things go really wrong. Don't you?
Not so! Truth is that even for the newest brands and ideas, people are discontinuing as other people are becoming true adopters. The more you can stem the tide of this discontinuance, the steeper your overall adoption (and sales) curve will be.
So if you're really serious about making a product launch successful, or perhaps trying to remedy a brand disaster, you need to have a proactive look at where and how your discontinuance will, or is, happening.
We've written a little paper about it which might give you a few more ideas, which you can download by clicking hereRead more....
The chart above is from a peer reviewed publication Babor E et al. Psychiatr Bull, 1996.
Look at how influential 'representatives' and 'advertising' are versus 'colleague recommendation', and contrast that with what's at the heart of traditional pharma marketing strategy. Read more....
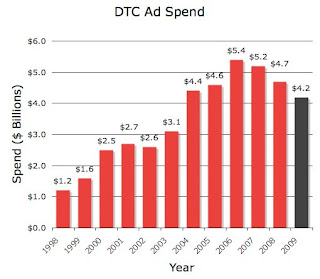
The chart above comes from this article on Pharma Marketing Blog. A first reaction would be to blame the downturn on the same thing everything else is being blamed on: the credit crunch / financial meltdown. However, the dip started in 2006, so while this may become a contributing factor, it isn't the main cause.
Anyone working in pharma will know that thinner pipelines and higher market access hurdles mean companies have been looking for efficiencies. My belief is that under this lens, traditional promotion - of which TV DTC has to be the most obvious example - is starting to look like the emperor with no clothes.Read more....
So far in this blog when it comes to the future of pharma marketing, I’ve mainly talked about us working to a better understanding of how pharma marketing really works - by adopting elements of diffusion theory and word of mouth (WoM) marketing.
There is another big change that’s already happening in pharma, and as with WoM it also shows how the consumer model aped for so many years is woefully inadequate – it’s Market Access.
“Back when I were a lad” learning the pharma marketing ropes in the 90’s, reimbursement and pricing was simple. The answer was always “premium price” regardless of the question. The only tricky bit was figuring out how much you could charge for something first in class. You called the pricing guys in at the last minute to do some research and put a price on it, and hey presto.
Such a scenario is clearly laughable today. As professor Michael Rawlins, head honcho and chief ball-breaker at NICE put it: “The industry has to accept that just because new drugs are licensed does not mean that the health service wants or needs to buy them.” Ouch. But as a tax (or insurance) payer though, you’ve got to admit he’s on the money.
I realise this isn’t news to many in pharma. These days we’ve all got departments focusing on ‘market access’ or ‘managed care’; some companies doing better jobs than others.
But here’s my challenge – how long should it stay like that; with a marketing department and a market access department? Sure, you might need a small army of people to go smoothing the numbers with to HMOs or Primary Care Trusts, but at a central strategic level there is no real division.
It’s still about marketing strategy, it’s just that we’ve finally added in price and access (volume) into the equation, along with the customers most interested in these points.
For us old-timers (hey, I’m still in my 30’s!), on first sight this can be a little scary: new customers with new jargon to deal with who seem hell-bent on not paying for our products. The way I like to think of it though is as one big negotiation and the fun bit is that it isn’t necessarily all about price.
Let me give you an analogy. I was talking to someone a few weeks ago who sold her car on ebay. By self-admission she is a neat-freak who had every skerrick of information on the history of that automobile, as well as a ton of photos detailing its condition. The car was in good order and so she put it on at a premium price.
In the auction it went at full asking price to a bidder who said that the reason they paid top-whack was because, sure it looked like a good car, but she was the only seller who had fully answered their gazillion questions and so they were comfortable to buy at that price.
The same thing can work with payers. Have the right data answering their troubling questions (like, just how much better than generics is it?) and you too can snap up a great price. Other levers to think about with your access strategy include the patient segment you’re going to target and proof of the buckets of money you can save them elsewhere in the system.
It takes a little practice to start getting this thought process in train, but rather than thinking of it as menacing hoodoo, we need to see it as a fun strategic challenge that’s part of the role. The “kids” growing up as product managers today no longer see the distinction. Get on board or get outdated – it’s the future I tells ya! Read more....